It’s True – Metals in a Tattoo – Systemic Contact Dermatitis
Yes, indeed metals can be implanted in a tattoo… and systemically activated reactions can occur in those tattoos related to those metals…
“We recommend assessment of permanent tattoos for inflammation in all patients undergoing patch testing, for additional diagnostic correlation.” [Dermatitis. 2008 Sep-Oct;19(5):E33-4]
Article 1 (came out yesterday) :de Cuyper C1, Lodewick E2, Schreiver I3, Hesse B4, Seim C5,6, Castillo-Michel H4, Laux P3, Luch A3. Contact Dermatitis. 2017 Aug 9. doi: 10.1111/cod.12862. [Epub ahead of print] Are metals involved in tattoo-related hypersensitivity reactions? A case report.
OBJECTIVES: We present a patient with papulo-nodular infiltration of 20-year-old tattoos associated with systemic symptoms that disappeared within a week after surgical removal of metal osteosynthesis implants from his spine. We aimed to explore the causal relationship between the metal implants and the patient’s clinical presentation.
METHODS: Metal implants and a skin biopsy of a reactive tattoo were analysed for elemental contents by inductively coupled plasma mass spectrometry and synchrotron-based X-ray fluorescence (XRF) spectroscopy.
RESULTS: Nickel (Ni) and chromium (Cr) as well as high levels of titanium (Ti) and aluminium were detected in both the skin biopsy and the implants. XRF analyses identified Cr(III), with Cr(VI) being absent. Patch testing gave negative results for Ni and Cr. However, patch tests with an extract of the implants and metallic Ti on the tattooed skin evoked flare-up of the symptoms.
CONCLUSION: The patient’s hypersensitivity reaction and its spontaneous remission after removal of the implants indicate that Ti, possibly along with some of the other metals detected, could have played a major role in this particular case of tattoo-related allergy.”
Article 2: Cobalt tattoo reaction:
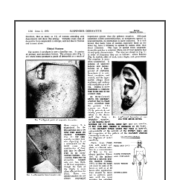
“An otherwise healthy 36-year-old Caucasian woman, without prior history of atopic dermatitis or eczema, presented to an outside dermatologist with a generalized, severely pruritic eruption involving the entire body except the face. One month previously, she had used a 50% trichloroacetic acid tattoo removal solution on a blue-colored tattoo on the medial aspect of the left ankle. The patient’s eruption persisted for 7 months, and after several attempts to slowly taper her prednisone dose, she presented to our institution. On physical examination, there was a 3-cm erythematous, lichenified plaque surrounding the tattoo (Figure). On the trunk and upper regions of the arms, there were scattered, 1- to 2-cm, nummular patches and plaques. Biopsy of a truncal lesion revealed spongiotic pustules with a mixed dermal infiltrate and scattered eosinophils, consistent with subacute spongiotic dermatitis.”
Article 3: Systemic Dermatitis following surgery — presenting as tattoo reaction
“We report three patients with permanent tattoos and chronic dermatitis. During patch testing, the patients’ dermatitis worsened, and the previously quiescent green-colored portions of the tattoos became inflamed. All three patients were patch-tested and had positive reactions to potassium dichromate 0.25% in petrolatum. Avoidance led to the resolution of both the dermatitis and the tattooinflammation. We recommend assessment of permanent tattoos for inflammation in all patients undergoing patch testing, for additional diagnostic correlation.”